By Lee Weingrad | Director, Surmang Foundation
Looking back on 25 years in Tibet
Steve and me
In the mid 90’s Steve Jobs went to New York to meet with some New York venture capitalists to fund the iPod. They asked him, “What kind of focus groups did you run?” Jobs replied, “What kind of focus groups did Gandhi run?” They asked again, “how do you know they’ll like it?” He replied, “They don’t know they want it yet.”
While I’m no Steve Jobs, I faced exactly the same kind of questions in establishing healthcare in E. Tibet. What kind of capacity do you have? What are the established needs? I was not a public health professional and while I knew none of the answers, I was confident we would succeed. And succeed we did.
The 4000 m alpine summers of Surmang are short and glorious, aromatic deep green fields abundant with wildflowers and wildlife. Snowcapped mountains glistening with sunlight rising on their horizon frame the scene.
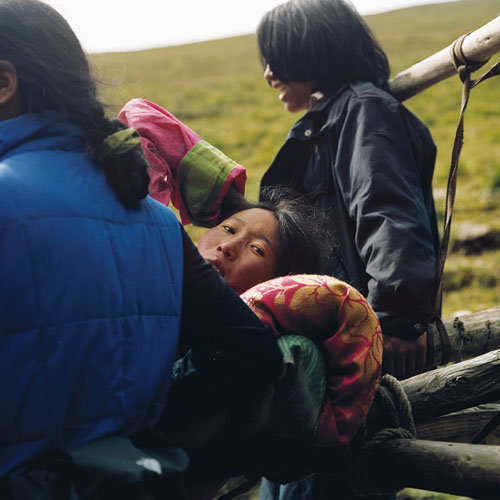
In 1991 we made out first trip with volunteer doctors to Surmang. It was 4-wheel drive country, with no roads and rivers and with no bridges. But the local response was breathtaking. No one had ever gone to so much trouble before to take care of them. Hundreds of people would come to our tent to be treated. Every day. While their personal response was very warm, none of them had ever seen more than one foreigner before. Me.
One of our doctors, David Dubin, said, gesturing to a Khampa warrior with long braided hair and a sword, “I feel like I landed on another planet.” I responded, “Imagine how they feel when they see us!”
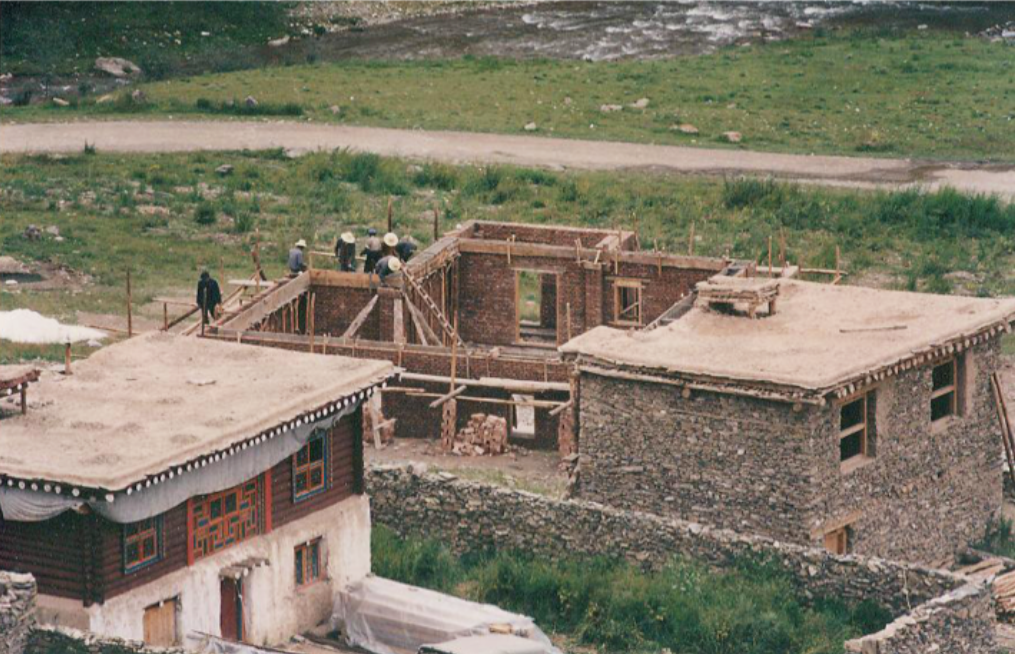
We continued. In 1992 we signed a partnership agreement with the Qinghai Prefecture government to build a clinic. Within 6 months we had the funding from Caritas. Three years later 1996, the clinic was finished. By 2000 we had a local Tibetan who completed 3-year-post-HS training as a doctor. By 2001 we had a second, a female. That summer our overseas volunteer doctors began a journey that continues today: training our two doctors.
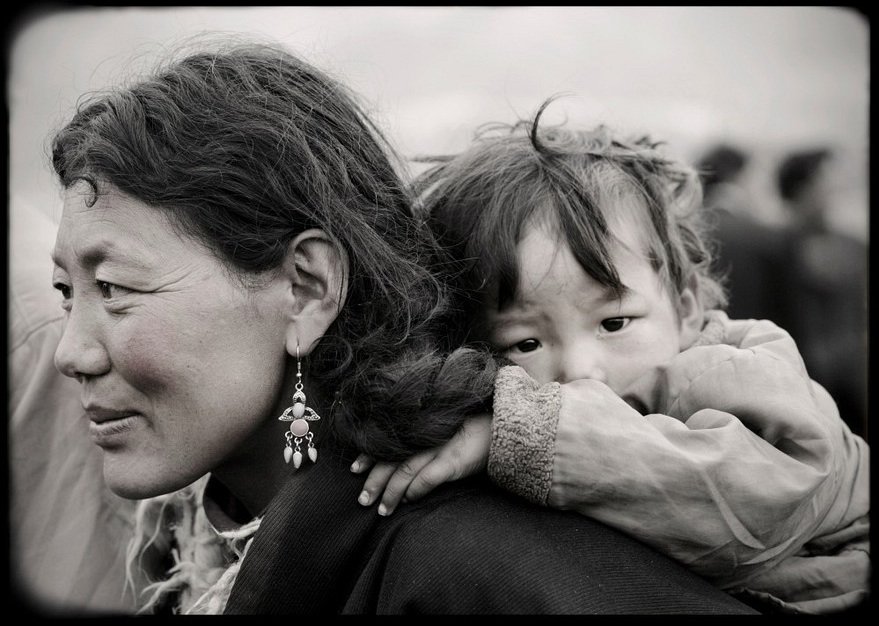
Throughout those first years of the 2000’s volunteer doctors like Julie Carpenter of Boulder, CO, would ask, “Why are there no women and children in this clinic?” That question was a game-changer. As a result we shifted our focus to mother and child health.
In ’94 we penned an agreement with the Yushu Prefecture Government to do a mass-data survey of 400 nomadic mothers. This is China and foreigners don’t run around surveying the locals. It had never done before, hasn’t been done since.
We found out that the region has one of the highest maternal mortality records on earth, on the level of Uganda or Somalia. I found out later that WHO estimates 6000 women die each year from childbirth or pregnancy. And they didn’t count Qinghai or Sichuan. The biggest threat to Tibetan health was facing death in the process of making life. The next year, 2005, with the cooperation of the government, we began to train 40 Community Health Workers, women embedded in their villages and nomadic camps to pro-actively remove the sword of Damocles hanging over the neck of every Tibetan mother and girl.
By 2011 maternal mortality in our area went to zero. And stayed close to there.
This year, 2016.
This year’s report will come at the end of November. Anecdotally I can report that among our clinic’s 9000+ patients treated for free and the region’s 95+ births, there were only 2 maternal mortalities and 1 infant mortality.
In the early 90’s Suzie Jolly, then with UNICEF asked me when we were building our clinic, “how do you know you will get any patients?” I asked her if she saw the movie, “Field of Dreams.” In that movie Kevin Costner’s character is asked to build a baseball field in his Iowa corn field so that the ghosts of the corrupt Chicago Whitesox (the “Blacksox”) could play an honest game and redeem their souls. He said, “How do I know they will play if I build the field?” The ghost said, “build the field and they will come.” I repeated this story to Ms. Jolly.
Two years ago I was re-connected to her through the late Maurice Strong. He said, “Call her up.” And so I did. When she answered the phone and I identified myself, she said, “build the field and they will come.”
Our work is to save Tibetan culture. If you want to save a culture, save a mother. We get no funds from foreign governments or churches or big foundations. We are driven by individual donations. There is one big takeaway for our many small donors: the feeling stays with you. Help us. See what happens.
Links:
By Lee Weingrad | Director, Surmang Foundation
By Lee Weingrad | Project Leader
Project reports on GlobalGiving are posted directly to globalgiving.org by Project Leaders as they are completed, generally every 3-4 months. To protect the integrity of these documents, GlobalGiving does not alter them; therefore you may find some language or formatting issues.
If you donate to this project or have donated to this project, you can receive an email when this project posts a report. You can also subscribe for reports without donating.