By Julia Downing | Project Leader
The Palliative Care Education and Research Consortium (PcERC) present this report highlighting activities and achievements during the past four months. Throughout this time, PcERC remained dedicated to providing holistic palliative care services to individuals living with life-limiting illnesses across Uganda. The program focused on both adult and pediatric patients, aiming to enhance quality of life through effective symptom management, psychosocial support, and family-centered care.
PcERC continued to collaborate closely with Mulago National Referral Hospital and Kiruddu National Referral Hospitalto strengthen access to specialized palliative care through well-coordinated referral systems. Service delivery at these facilities was supported by a multidisciplinary team composed of six PcERC staff members, three public health professionals, seven volunteers, and one representative from Makerere University. This team structure enabled efficient coordination of services and ensured continuity of patient care.
During this time, PcERC delivered specialized, evidence-based palliative care to 205 patients, including 24 children under the age of 18. In addition, 575 family caregivers received education and support to enable them provide ongoing care at home. Of the patients served, 82 were male and 123 were female. A total of 142 patients were diagnosed with cancer, while 63 were living with non-cancer conditions requiring palliative care support.
Although efforts continue to promote early referral, 66 patients died, largely due to late presentation and advanced disease at the time of referral. However, 139 patients improved and were discharged, with appropriate linkages established for continued care. Among those discharged, 61 were referred to hospices or community-based palliative care providers, 42 were referred to the Uganda Cancer Institute for specialized oncology services, and 36 patients with non-cancer conditions were referred back to nearby health facilities for follow-up care. Unfortunately, twelve patients were unable to continue treatment because of severe illness, financial limitations, or lack of appropriate services. During the reporting period, the team recorded 7420 direct in-person patient contacts.
To strengthen continuity of care beyond hospital visits, PcERC continued to utilize digital communication platforms. Through regular phone calls and WhatsApp, the team-maintained contact with patients and caregivers to monitor symptoms, provide guidance, and ensure patients were able to access follow-up services through established referral pathways. A total of 4,260 telephone consultations were conducted during this period. These interactions also provided opportunities to offer emotional support and bereavement counseling to families who had lost their loved ones. The dedication of the clinical team remains central to these achievements, as they continue to provide compassionate care that addresses the physical, emotional, and spiritual needs of patients and their families.
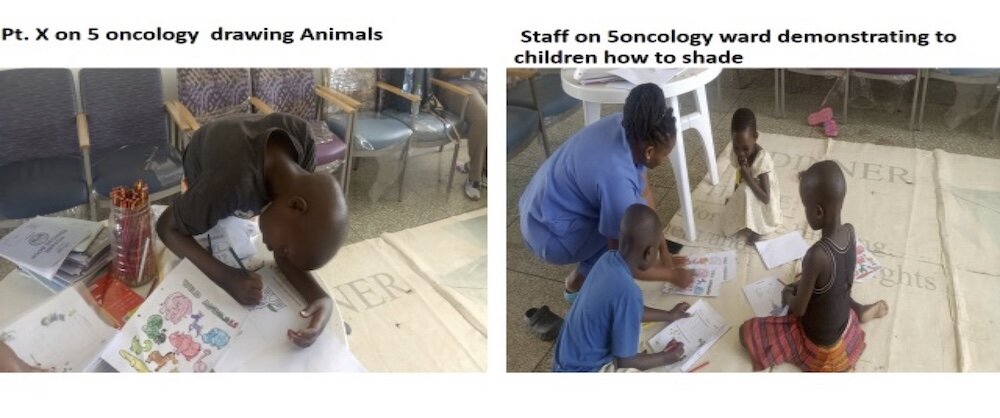
Pediatric palliative care continues to be an important component of the program. A total of 24 children were followed up through an initiative conducted in collaboration with the African Palliative Care Association. Within this study, the Children’s Palliative Outcome Scale (CPOS) was used to assess and monitor the needs of the children. Through this program, seven children were identified and enrolled for specialized pediatric palliative care interventions. This collaboration has enhanced the capacity of the Palliative Care Education and Research Consortium (PcERC) to recognize complex pediatric palliative care needs and to deliver improved, responsive care for children living with serious illnesses.
Additionally, our symptom management protocols and clinical modelling empowered link nurses and general practitioners to handle 320 patients in the hospital, across different wards. From these, 82 we receive consultations for specialist palliative care input, though 31 unfortunately passed before consultations, typically due to after-hours or weekend constraints.
Restoring Hope in Difficult Circumstances: A Story of Impact
Even in situations that may seem overwhelming or without hope, palliative care services continue to offer comfort, dignity, and support to patients and their families. Through compassionate care and dedicated support, many lives are touched and transformed. The following story highlights the meaningful impact of these services.
Story 1: When Compassion Becomes Family: The Lifeline of Palliative Care Volunteers
Patient J, a 54-year-old man with cancer of the oesophagus, entered palliative care alone. With no caregiver or family support, his illness stripped away not only his physical strength but also his sense of belonging. Painful swallowing, weight loss, and weakness left him unable to work or care for himself. Hospital visits filled him with anxiety, and practical needs—transport, food, medication—became overwhelming. Beyond the physical burden lay an even heavier emotional one: loneliness, fear of dying alone, and the belief that he was a burden to the healthcare system. His story reflects the plight of many patients who face serious illness without family or community support.
Palliative care volunteers stepped into this void, becoming the consistent human connection he desperately needed.
These interventions transformed his quality of life:
Patient J’s story is not unique. Across communities, countless patients face serious illness without caregivers or family support. Volunteers become their lifeline—bridging gaps in care, reducing suffering, and restoring dignity. Ronald is a committed volunteer who diligently supports patient J. he is currently pursing a degree in social work to build and develop his skills.
When compassion becomes family, despair turns into dignity. Patient J’s journey shows that volunteers are not an optional addition to palliative care—they are essential. By supporting and scaling volunteer programs, you are helping to ensure that every patient, regardless of family circumstance, experiences comfort, connection, and humanity at the most vulnerable time of life.
Education
We continue to prioritise training and mentorship for both undergraduate and postgraduate learners from various universities and institutions, with the goal of enhancing knowledge transfer, building practical competencies, and promoting the integration and sustainability of palliative care services.
Over the past four months, clinical placement opportunities were provided to undergraduate students from Makerere University (118) and the Islamic University in Uganda (80), as well as diploma students from ENT (35) at both basic and post-basic levels.
Through structured mentorship, hands-on clinical exposure, and ongoing support, learners are equipped with the necessary skills and confidence to apply palliative care principles effectively in their future professional roles.
In addition, PcERC has strengthened the capacity of its staff and volunteers through continuous professional development. This has resulted in a highly skilled and competent team capable of delivering quality services in patient care, education, and research.
Research
We continue to conduct studies to promote evidence-driven approaches and advocacy. Our partnerships encompass the University of Coimbra, Oslo University, University of Sheffield, APCA, and King’s College London. We have completed data collection of the University of Coimbra; PARA STOP and the C-POS initiative we finalizing with reports.
Advocacy and Sustainability
To achieve sustained impact and expanded reach, PcERC continues to prioritize advocacy and sustainability efforts that highlight the value of palliative care across Uganda. Between October and January implemented a range of awareness campaigns, Continuing Medical Education (CME) sessions, and joint activities with local health authorities to promote public understanding of comprehensive end-of-life care.
These initiatives helped to dispel misconceptions surrounding palliative care while strengthening collaboration with key stakeholders, including the Ministry of Health and various non-governmental organizations, to support its integration into national health frameworks.
To promote sustainability, we emphasized capacity building for primary care ward teams through structured mentorship programs and pursued diverse funding opportunities, including grant applications. This approach has enhanced our organizational resilience, allowing us to maintain service delivery despite limited resources. We also acknowledge and appreciate the support of GlobalGiving, whose partnership continues to strengthen these advocacy efforts and extend care and hope to more families in need
Conclusion
During the past four months, the Palliative Care Education and Research Consortium (PcERC) demonstrated sustained commitment to improving the quality of life for patients with life-limiting illnesses and their families. Through collaboration with key institutions such as Mulago National Referral Hospital, Kiruddu National Referral Hospital, the Uganda Heart Institute, and the Uganda Cancer Institute, the program continued to deliver compassionate, patient-centered care addressing physical, emotional, social, and spiritual needs.
By Julia Downing | Project Leader
By PcERC Team Members/ Julia Downing | Project Leader
Project reports on GlobalGiving are posted directly to globalgiving.org by Project Leaders as they are completed, generally every 3-4 months. To protect the integrity of these documents, GlobalGiving does not alter them; therefore you may find some language or formatting issues.
If you donate to this project or have donated to this project, you can receive an email when this project posts a report. You can also subscribe for reports without donating.
Support this important cause by creating a personalized fundraising page.
Start a Fundraiser