![]()
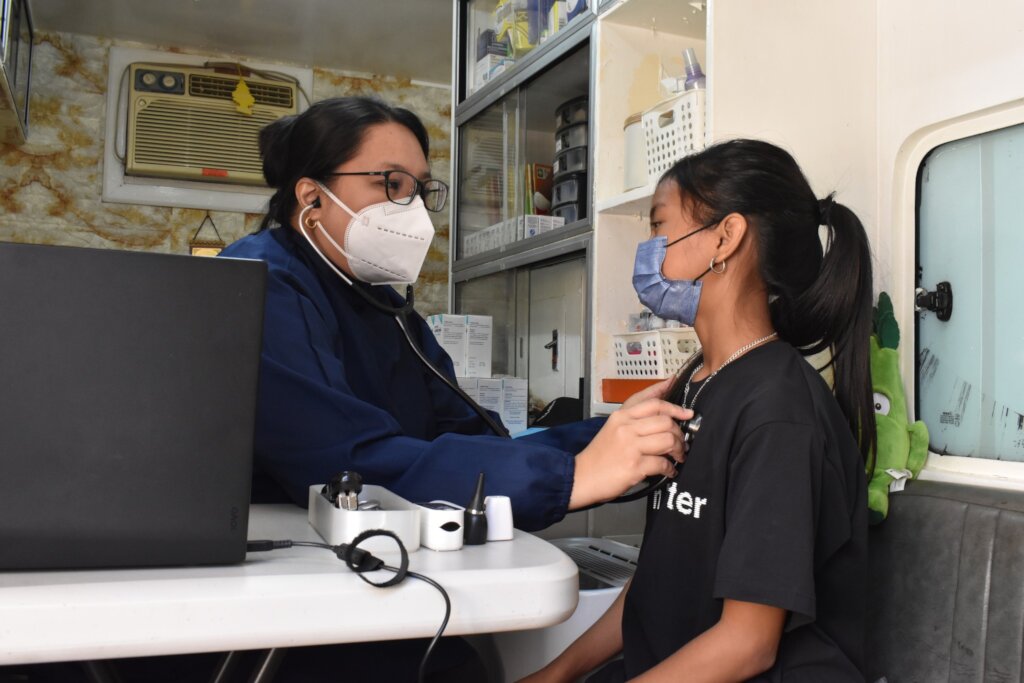
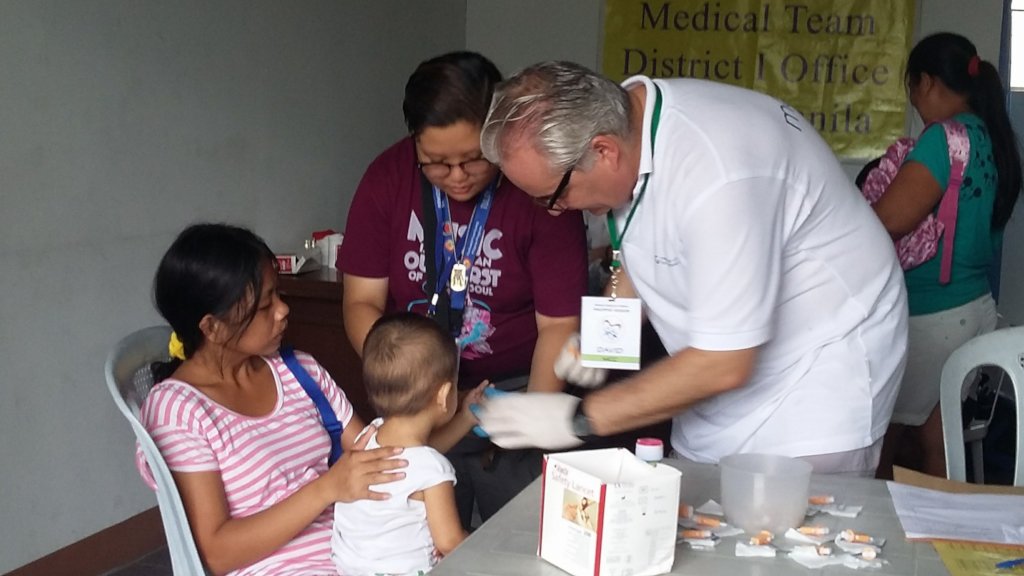
Childhope Philippines continues its drive to eliminate intestinal parasitism in street children of Metro Manila. The Childhope’s Mobile Health Project in partnership with school volunteers are distributing anti-helminthic drugs during the National Deworming Month (NDM) campaign of Department of Health, held last December 19, 2018 at Museo Pambata, Manila.
Deworming is being done because Soil Transmitted Helminths (STH) is a public health problem that has detrimental impact on children’s growth and development. STH can cause anemia, malnutrition, weakness, impaired physical and cognitive development resulting to poor growth and school performance in children.
The magnitude of the problem of STH showed that 6 out of 10 pre-school children ages 1-5 years old (baseline prevalence of 66%) (2004, DOH-UP-UNICEF) and 5 out of 10 children (54%) aged 6-14 years old (2003, UP-CPH) were affected with STH. Recent data also showed that the overall prevalence of STH among school-age children is 28.4% with 13 Regions still having prevalence of more than 20% (DOH-RITM National Parasite Survey, 2013-2015).
The World Health Organization (WHO) set the target that at least 75% deworming coverage should be attained but the Department of Health has a higher target which is 85%.
Last December, the deworming coverage among 30 street children under the assistance of Childhope Philippines has been dewormed.
“Childhope Philippines together with its partners and volunteers continues the initiative of conducting the deworming to achieve our goal in reducing the prevalence of Soil Transmitted Helminths in the country to less than 20% by 2022 to prevent its detrimental impact on children’s health and education if not properly addressed or treated.” Mobile Health Project Officer, Dr. Josefina Carpio stated.
University of the East Ramon Magsaysay Memorial Medical Center, Inc., who has sent volunteers and has donated 1,500 tablets of Mebendazole which will be used to deworm all five to fourteen year old street children under the Mobile Health Program of Childhope Philippines.
“It’s our commitment to foster a healthy community that will address public health challenges like the STH, with a goal to improve health and nutrition of impoverished children in the country,” said Ralph Lorenz apilado, UERM Volunteer
”We ask for the support of the parents and guardians to support this great endeavor. The success of this campaign relies profoundly with the support and actions of the non-government organizations, developmental partners and the local government units. With this unified effort, health for all will be achieved” Dr. Carpio concluded.
![Share on Twitter]()
![Share on Facebook]()