By Margaret McGlynn Reynolds | CEO, Co-founder, Vice President
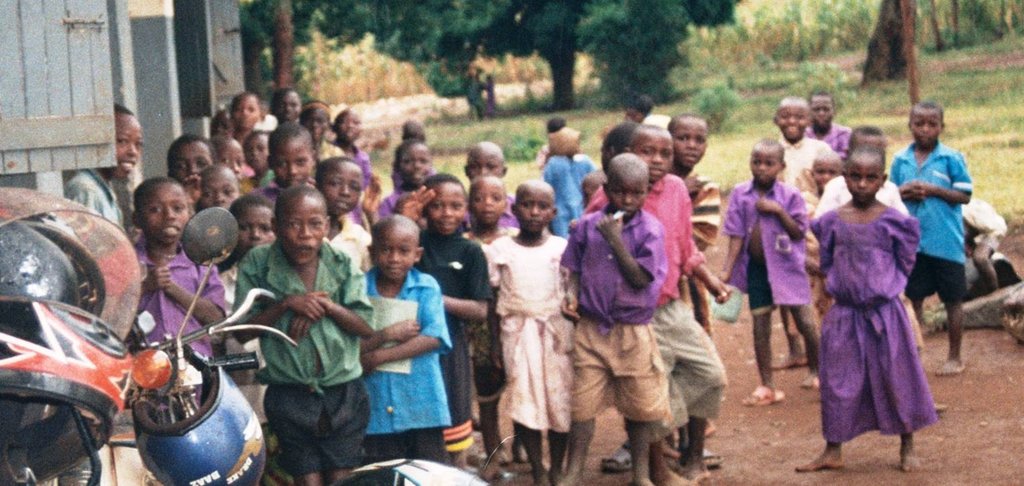
Walking down 70TH Avenue, I instinctively pulled out my iPhone to take a photo, document this scene to show people back home. Then, I stopped. I was home, but spending as short as 4 weeks without electricity or indoor plumbing, showering with buckets, cooking with firewood, walking to town to charge a phone is enough to make you feel like a visitor in your own home after returning. Walking to my marble-floored hospital down a crowded, concrete sidewalk, bumping shoulders without any apologies, any greetings, could not have been more different from my commute to Katulikire Health Center. I walked down a red, dirt path, past mud huts, barefoot children walking to school in uniform, barefoot children carrying jerricans of water in tattered clothes back home, women water in arms, firewood on head, baby on back. Naked tottlers waddling back toward the security of home, afraid by my pale skin. Children smiling, greeting me, but everyone so obviously poor, and so obviously in need.
I arrived to the Little Sisters of Mary Immaculate, Gulu convent to meet six sisters—one more enthusiastic and smiley than the next—and I was shown my room. “I can’t stay here,” was my first thought after being escorted to the outhouse where holes served as toilets, the room with lizards on the ceiling. I was provided with a jerrican of water and a flashlight for lighting. Yet, I couldn’t complain to anyone. It took about 24 hours for me to realize that I was staying in the nicest accommodations for at least 30 miles.
The health center didn’t have electricity, it didn’t have running water. Women labored on plastic tarps, which were rinsed and laid out for the next mother, nurses delivered their babies wearing only “sterile” gloves for protection. In the sick ward, babies, children, and pregnant women were cared for by relatives who cooked with fire in a covered shelter. The clinic did not have a doctor on staff. There were few medication choices, few lab tests. But I quickly realized, that those things were rarely needed. The most common outpatient visit and inpatient hospitalization was due to malaria. Malaria is not always malaria at such understaffed and poorly resourced clinics. Clinics exist where every diagnosis is malaria, but this clinic only diagnosed malaria with a positive blood smear—a highly advanced practice for such an underprivileged clinic.
Everyone gets malaria almost annually. For those who do not succumb to the illness, they are knocked off their feet for a week or more with profound weakness, diarrhea, headache, etc. Because it is so widespread and devastating, malaria cripples development in numerous ways. There is 16-year-old Gloria who came in as an outpatient in the middle of her high school midterms. In Uganda, it is believed that students should learn the entire semester and understand concepts; illness during midterms should not impact performance. If Gloria didn’t perform, she won’t be back in high school next semester. There is 2-year-old Florence whose father was recently disabled by an accident, and her older sister, seven-year-old Scovia, pulled from school to stay home to help with the sustenance farming. The family has no money, which has been further complicated by the fact that Florence is very sickly. This recent case of malaria further weakens Florence and prolongs Scovia’s absence from school. Scovia has only completed first grade. A child who becomes a teenager with a first grade education level will surely be married early and become a teen mother herself. There is 16-year-old Sharon who dropped out of school, she was married to a man, and expecting their first child. She came to the hospital and delivered a child 6 weeks premature, she fell into a coma and was taken away by her family to likely die—all from malaria.
Insecticide-treated malaria nets do work. It is difficult to find them in such a poor area of Uganda, and even if they’re given out, it can be difficult to convince people to use them. Because of this difficulty working with adults, we have begun targeting school children. Providing nets to school children gives us the opportunity to thoroughly educate them about the cause of malaria, how to prevent it, and how to use nets. I was surprised to learn that many adults do not know that mosquitos carry the parasites that cause malaria. When talking to even the most educated adults, they said that they preferred to sleep without nets that make them hot and take their chances with malaria. School children do not feel the same.
Distributing nets to school children is also very important because we are working with a group of people who do not always send their kids to school. Public schools in Uganda are free, but thousands of children register for school in Katulikire area and never attend. Our children are the children of refugees and internally displaced persons. The adults have survived horrific wars. Every family has stories of themselves being abducted as child soldiers, sex slaves, or siblings suffering in such ways; watching parents, relatives, neighbors burned alive in huts. They spent their childhood running for their lives. They never benefitted from education. Over 75 percent of women who come to the health center sign with a fingerprint meaning that they can’t read or write well enough to sign their own name. Convincing these parents—who have never met anyone with a college degree, have never met anyone with enough money to build a home with electricity or indoor plumbing—that they should keep sending their child to school, is a difficult task. Rewarding the children for coming to school by giving them a malaria net, incentivizes them to continue coming, and encourages parents to send their other children to school. “Good things are happing to those who go to school.”
While in Uganda, I had the privilege of distributing about 5,000 nets to 5 grade schools. The teachers thanked us for our hard work endorsing the number of absences from malaria saying that our efforts will keep their children healthy and keep them in school. We distributed nets to Okwece, a school with over 1,000 students who anxiously awaited our arrival. One of the teachers, so grateful that we had come, brought us back to his home, killed an entire chicken which he fed to us while he and his wife watched from the doorway with their hungry children and starving dog, waiting for leftovers before themselves eating.
We distributed to Karungu II, a school just off of the Nile River, with a very high malaria burden. The school has grown with attendance so much that there is not enough space in the buildings. One class is held under a tree. Another class takes place under a large, thatched roof supported by trees.
We distributed to Kothongola, a school with incredibly poor attendance. Of the 1000 registered students, about 400 were in school. Kothongola is an area where the children are kept home to help on the land. Hopefully, bringing nets to Kothongola will lead to increased attendance.
Mutunda is a really good school. It has produced many of the area’s politicians. The culture of the school values attendance and education. It also pushes the teachers to teach well and advocate for their students. An investment in Mutunda is an investment in the future leaders of the Katulikire area.
Kakokwo is a typical Katulikire school with a separation between those students who attend vs. those who do not attend. Those who attend can help us get those who do not attend to school.
Finally, I had the opportunity to meet many children who had received our nets in the past. Some even took us to their homes—huts with grass roofs, dung floors, surrounded by chickens and pigeons. Jennifer, a sixth grade student at Opok Primary School sleeps on the dung floor of her hut with her baby. She was sent away to boarding school and “deceived” by a man and conceived a son. She is now back at Opok struggling to stay in school. Our net, which she and her baby sleep under on the dung floor, helps her and her son, now 7/8 months old stay healthy, save money on medical costs, and stay in school. Molly, a sixth grade student whose father was murdered last year, also thanked us for her net. Without a living father to provide for her, it is a great struggle to stay in school. At least she does not have to pay for treatment for malaria. We also visited previous recipients at Katulikire, St. Monica, etc. Everyone thanked us profusely. They are protected from malaria, so their families do not have to spend so much money on treatment. The extra money enables them to stay in school, and allows their families to spend the money on other basic needs, like buying food or buying seeds.
Having now been back in the US for awhile, it’s very different here. Walking around Katulikire, there is a palpable feeling of pain and suffering. The feeling on the streets of the US is so different. Despite their suffering, the Ugandan villagers were most generous to me. I was given plots of land, looms of Ugandan fabric, a hand-made dress, skirt, gifts for my family. I was always a celebrated guest often going to a village home where I would be fed until I was so full I was gagging. Villagers walked for hours to bring me gifts. These gifts were given from what they did not have. It made my sacrifice to live four weeks without electricity and indoor plumbing seem minimal.
Still, their suffering is real. In these few short paragraphs, I have discussed numerous, seemingly insurmountable problems. It’s difficult to know where to start. I believe the lowest cost, most effective intervention is working with malaria prevention. Malaria kills, stifles education, cripples the workforce, and drains financial resources. We are working to expand our efforts and impact in Katulikire. I would like to work with education; I would like to work with the mothers. For now, I am convinced that the community will never improve without better control of malaria. I could not be more grateful for your generosity to my friends in Uganda. I know that you have many needs, see many needs and your sacrifice may not be so different from that of my friends in Katulikire who did my hair, hung beads around my neck, prepared a rabbit, scaled trees to pick fruits and watched proudly, joyously, but hungrily as I ate because there was not enough to go around.
By Margaret McGlynn Reynolds | CEO, Co-founder, Vice President
By Margaret McGlynn Reynolds | Vice President, CEO
Project reports on GlobalGiving are posted directly to globalgiving.org by Project Leaders as they are completed, generally every 3-4 months. To protect the integrity of these documents, GlobalGiving does not alter them; therefore you may find some language or formatting issues.
If you donate to this project or have donated to this project, you can receive an email when this project posts a report. You can also subscribe for reports without donating.