By Lee Weingrad | Director
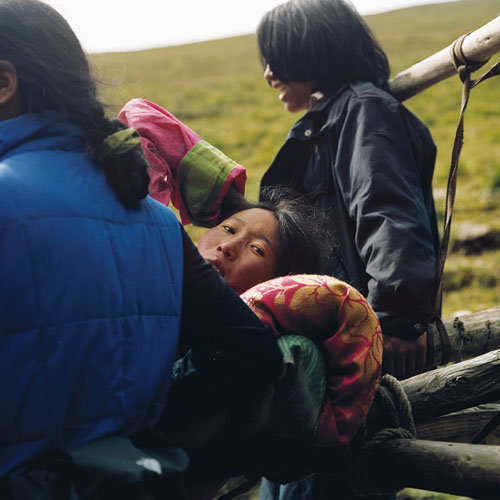
The winter months are quiet ones for our programs but not for our clinic projects nor the Khampa Tibetan patients. In October, the snows come down to about 3500m, the nomads fold up their sturdy yak hair tents, and with their herds of yak, horses and goats go to the lower elevations, to their villages and permanent homes. By December the passes close. The Surmang Clinic, the Community Health Workers and the 4 township hospitals are snowed in. For a time when the passes are closed, with days short, the families stay warm around the yak dung stoves eating tsampa and yak jerky, drinking salty butter tea.
For patients who are not facing life or death crises, wintertime brings farmers and nomads closer proximity to medical help than in the summer when the nomads are disbursed among the remote alpine encampments. This is good news for any kind of sub-acute problem. But for problems that require evacuation it is difficult. But for women and children who need early intervention the clinics are closer than in the summer.
Higher skill levels for providers and early intervention. That is the key.
Increasing the skills of these providers in ways they can use, and linking up these folks –village health workers to village doctors, village doctors to township hospitals—that’s the way you create a system with synergy. That is why we are building birthing centers this summer with the help of the Danish Chamber of Commerce, China. But the hardware, the bricks and mortar only take us so far. We need support from you through globalgiving.org to pay for the training of these rural doctors, to enable them to use these facilities.
And that is the reason we’ll have a much bigger training of village docs and village health workers this summer than ever before. It sounds simple, but actually the directness and lack of jargon-driven agendas makes us outside the box of conventional development and public health approaches.
In the winter we too, at Surmang Foundation sit around our virtual fire, a period of regrouping, planning and strategizing. We can’t travel to East Tibet to oversee projects so we design for the coming year, we recruit the volunteers who will work on these projects, and we raise the funds we need for the whole year. So we must plan carefully to use our resources carefully. That’s where you, the donor come in.
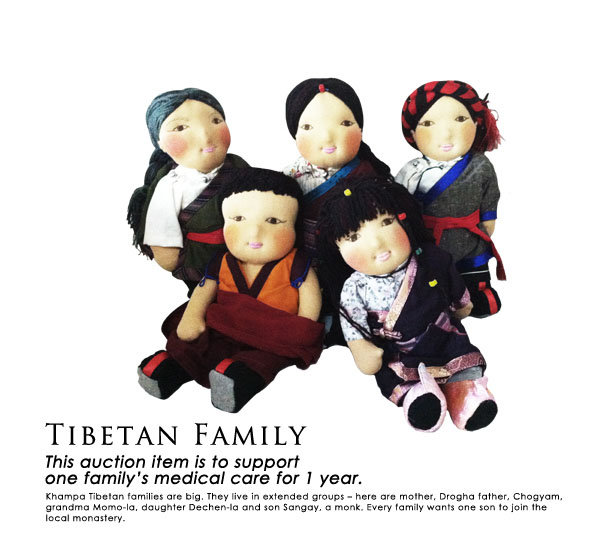
In the November Beijing Fundraiser we auctioned off a “Tibetan Family” in the guise of dolls donated to our cause. The winning bid on the families represented the cost of providing medical care to a family. We were very successful, raising over $4,000 for each “family.” I encourage anyone who wants to participate at this level to make such a donation.
2014 promises to be a big year for us –we so far have 4 volunteer doctors including the return of our own esteemed Dr. Julie Carpenter. We’re going to visit once again the Shechen Orphanage and offer medical services there.
Suzanne Smith, a veteran of over 10 years in community organizing in Africa will join us as a project manager. Janis Tse yong-jee will return. The Chinese community is rising to the challenge – there will be a fundraiser in March. We are now registered in Qinghai Province. We are hoping for national registration by the end of the year.
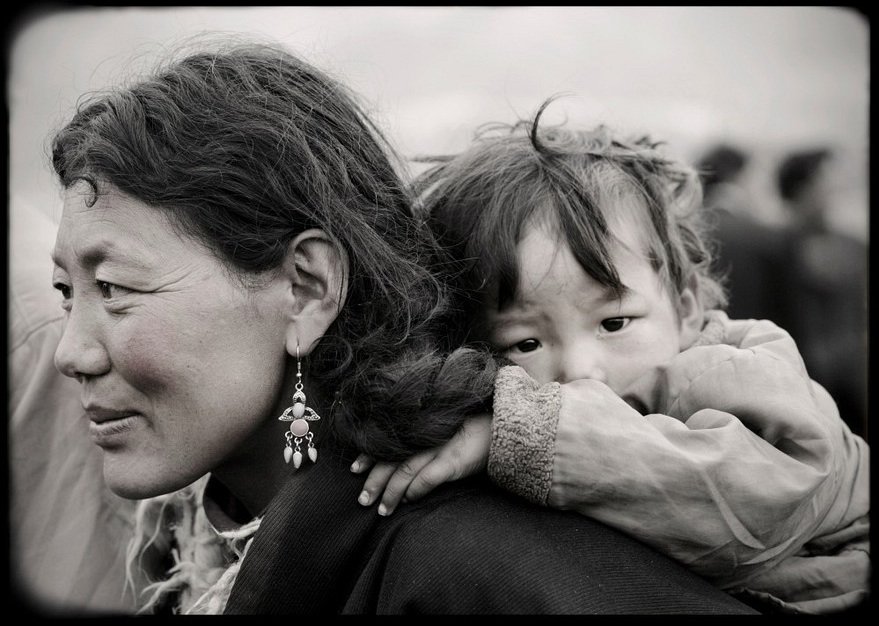
It feels like our resources are gathering. Our calling is the stuff of life –and death—mothers and babies who carry the future of Tibetan families and Tibetan culture. So in the words of the poet, we have promises to keep and miles to go before we sleep. Please help.
Links:
Project reports on GlobalGiving are posted directly to globalgiving.org by Project Leaders as they are completed, generally every 3-4 months. To protect the integrity of these documents, GlobalGiving does not alter them; therefore you may find some language or formatting issues.
If you donate to this project or have donated to this project, you can receive an email when this project posts a report. You can also subscribe for reports without donating.