By Kim McCloud | RCOG International Fellow
I am the first RCOG fellow working at Mbarara National Referral Hospital in Western Uganda. It is a 600-bed teaching hospital, affiliated to the Mbarara University of Science and Technology, one of four medical schools nationwide. There’s a large obstetrics and gynaecology department of 7 consultants, 15 registrars, 2 house officers and 20 midwives. The hospital has approximately 8000 deliveries a year with a Caesarean section rate of 30%. Through implementation of critical incident reporting and an increased number of residents the unit has reduced its maternal mortality rate from 722 in 2009 to 325 per 100,000 in 2011, with the primary cause of death being sepsis.
I arrived at Entebbe airport and was driven the 174 miles to Mbarara. My accommodation is conveniently located across the road from the hospital and has security guards at all times. It is a self-contained flat with all the essentials. The Ugandan power supply is currently insufficient to meet the needs of such a rapidly-developing country, and there are frequent power cuts. Consequently, a head torch is essential to help you get on with things in the dark.
In the hospital I have found the staff to be incredibly friendly and helpful. The pathologies I have encountered thus far have been very different from those I encountered in the UK, with a high incidence of malaria and eclampsia. There is a relatively high incidence of Caesarean hysterectomy, the majority of which are secondary to uterine rupture. Thankfully, compared to other parts of Africa, there is a low incidence of destructive delivery.
Inevitably, when working in a developing country, there are many frustrations. There are also many logistical problems with the delivery of Ugandan healthcare. It is not unusual for theatre lists to be cancelled because of a lack of clean drapes or gowns. The medical management of obstetric patients has also proved challenging. Women tend not to receive adequate doses of medication, generally due to a lack of organisation on an under-resourced ward. This results in patients receiving sub-optimal therapy for their malaria and sepsis, and induction taking far longer than it should.
I hope to improve maternal services in Mbarara through the introduction of clinical guidelines, starting with malaria management and induction of labour. I also believe that care can be enhanced by emphasizing the importance of regular medications and clinical examination. I also plan to equip the antenatal ward (which accommodates antenatal women and those in the 1st stage of labour) with screens to facilitate easier examination and patient privacy, and a patient board to clarify when medications and reviews are due to take place. Moreover, I am hoping to supply glucometers to the wards to enable monitoring of their diabetic patients and patients receiving quinine who are prone to hypoglycaemia.
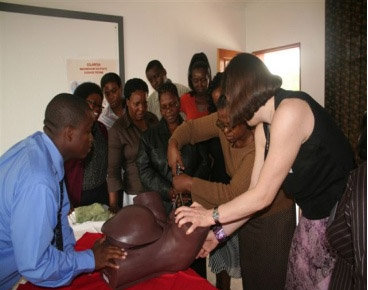
I have begun to offer regular teaching sessions which have focused on the management of obstetric emergencies and CTG interpretation for the residents, interns and medical students. I hope to expand this programme with assistance from the RCOG with their provision of mannequins to facilitate ‘hands-on’ teaching. I also plan to begin basic ultrasound training to help the doctors here assess viability, presentation, liquor volume and placental site.
I have also been in discussion with the hospital’s HIV clinic with the aim of piloting a scheme for cervical screening with VILI and VIA for these high-risk patients through our cervical cancer clinic.
It is not easy to facilitate long-lasting changes to the healthcare systems that exist here however with the support of the RCOG I am confident that by introducing small, step-by-step changes in the way that doctors here practice and train, I can contribute to a general improvement of the management of obstetric patients here in Mbarara.
Project reports on GlobalGiving are posted directly to globalgiving.org by Project Leaders as they are completed, generally every 3-4 months. To protect the integrity of these documents, GlobalGiving does not alter them; therefore you may find some language or formatting issues.
If you donate to this project or have donated to this project, you can receive an email when this project posts a report. You can also subscribe for reports without donating.