![X - Ray Irradiator - First in Asia Pacific]()
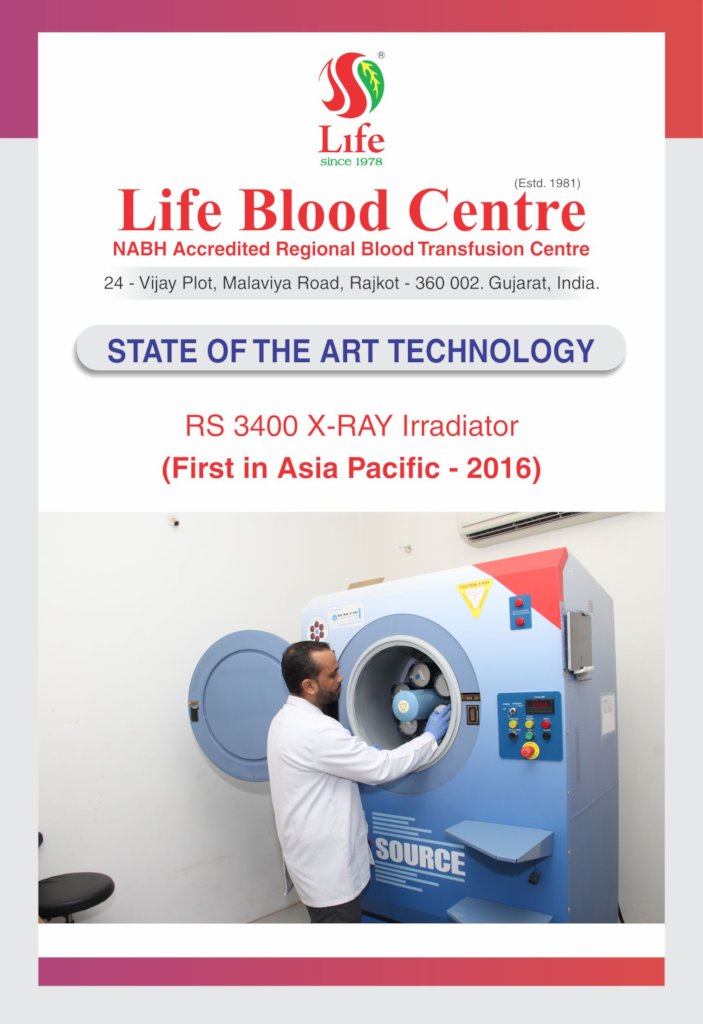
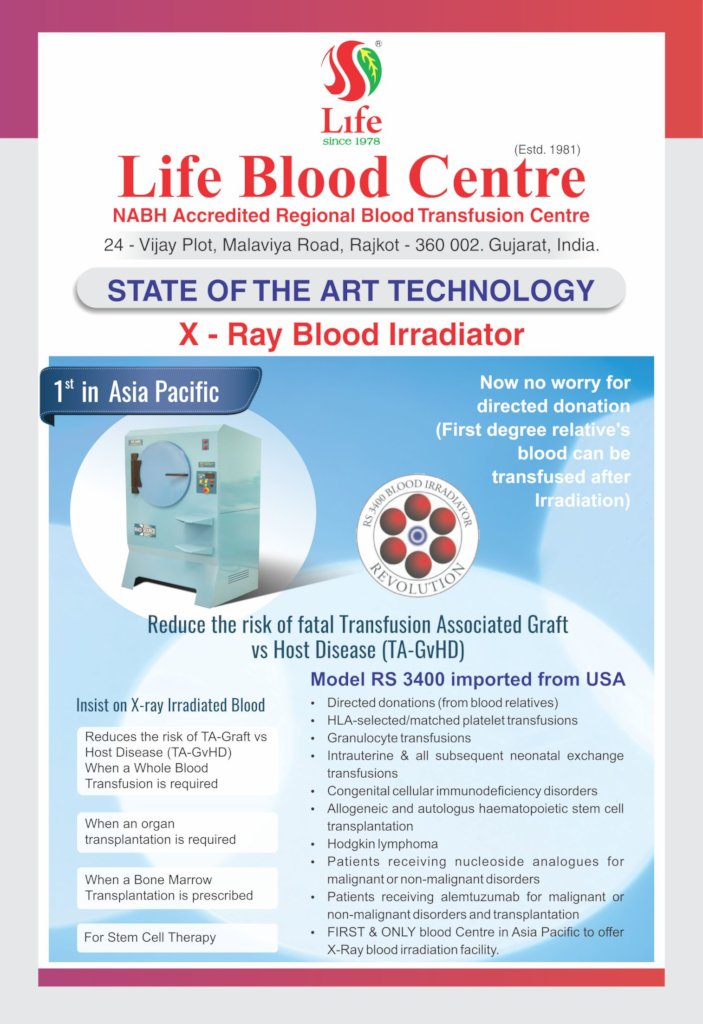
X - Ray Irradiator - First in Asia Pacific
IRRADIATED BLOOD PRODUCT....X RAY IRRADIATOR
TA-GvHD (Transfusion Associated Graft versus Host Disease) is a very rare but usually fatal complication following transfusion of lymphocyte-containing blood components. Although the first reports concerned cases where viable allogeneic lymphocytes had been transfused into immunosuppressed recipients, it became apparent that non-immunosuppressed patients could also experience this problem, particularly if the blood components they received came from an HLA haploidentical unrelated donor or family member.
The risk associated with an individual transfusion depends on the number and viability of contaminating lymphocytes, susceptibility of the recipient’s immune system to their engraftment and degree of immunological (HLA) disparity between donor and patient. The minimum number of transfused lymphocytes necessary to provoke a GvHD reaction is unknown and may vary by clinical settings. Until recently, gamma irradiation of cellular blood components has been the mainstay of TA-GvHD prevention but now X-Ray IRRADIATION cellular blood products are getting into practice.
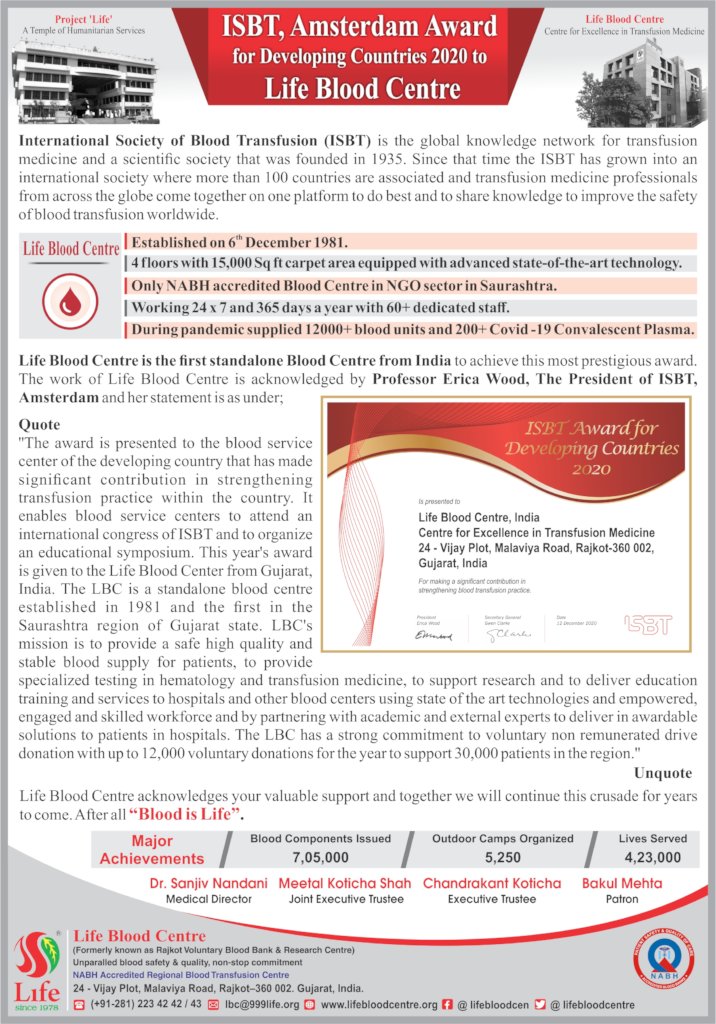
Fortunately, first installation of X-Ray irradiator of South-East Asia is done in Rajkot at Life Blood Centre.
Pathogenesis, clinical features and diagnosis of TA-GvHD
Pathogenesis:
TA-GvHD is a potential complication of transfusion of any blood component containing viable T lymphocytes when there is disparity in the histocompatibility antigens between donor and recipient. As well as the classical skin, gut and liver involvement seen in GvHD occurring after allogeneic stem cell transplantation, TA-GvHD is characterized by profound marrow hypoplasia and mortality in excess of 90%. There is a particular risk of TA-GvHD when the donor and patient share an HLA haplotype, as occurs within families, or in populations with restricted haplotype diversity In the Japanese population, the incidence of TA-GvHD is 10–20 times higher than in the North American Caucasian population.
Clinical features:
The early features are fever, maculopapular skin rash, diarrhoea and hepatitis occurring 1–2 weeks after transfusion. Bone marrow involvement produces severe hypoplasia with profound pancytopenia.
Diagnosis:
Diagnosis is usually made by biopsy of skin, gut or liver supported by evidence of persistence of donor lymphocytes. The presence of cells of donor origin may be demonstrated by polymerase chain reaction in peripheral blood (Utter et. al., 2007) or short tandem repeat analysis using peripheral blood and skin biopsies from affected and non-affected sites in the patient, and peripheral blood samples from the implicated donors.
Prevention of TA-GVHD
Irradiation
The major technology for preventing TA-GvHD is irradiation of blood components to inactivate residual lymphocytes Gamma rays and X-rays are similar in their ability to inactivate T lymphocytes in blood components at a given absorbed dose. Gamma-irradiators are expensive and eventual decommissioning and disposal present significant difficulties These highly radioactive cores may present a security risk in hospital settings. As the source decays, regular recalibration is required and irradiation time progressively increases. Dedicated X-ray blood irradiators are now available, have been widely used in North Americaand are being introduced by the UK Transfusion Services. X-ray irradiation machines are less expensive and the absence of a radioactive source results in fewer regulatory requirements. Published data indicate that the small differences in red cell permeability found between X- and gamma- irradiated components are not clinically significant. Further work, commissioned by the Joint Professional Advisory Committee of the UK Transfusion Services on blood components irradiated using the Raycell X-irradiator, concluded that gamma and X-irradiation can be regarded as equivalent and both are suitable and safe for clinical use.
Effective dose:
Studies using sensitive-limiting dilution assays indicate that a dose of 25 Gy, measured at the mid-plane of a component, completely abolishes mixed lymphocyte response.
The American Association of Blood Banks (AABB) recommends a dose of 25 Gy to the central area of the component with no portion receiving <15 Gy (AABB 2006). The Japanese Society of Blood Transfusion’s Guidelines recommend a similar dose. In the UK, a minimum of 25 Gy is recommended, but with the dose to any bag in the container not exceeding 50 Gy. To ensure this dose distribution is achieved, consultation with supporting physicists is mandatory.
Blood components that should be irradiated
Lymphocyte viability is retained in stored red cells for at least 3 weeks and TA-GvHD has been reported after transfusion of whole blood, red cells, platelets and granulocytes .TA-GvHD has not been described following transfusion of frozen deglycerolized red cells, which are thoroughly washed free of leucocytes after thawing.
TA-GvHD has not been described following transfusion of cryoprecipitate, fresh frozen plasma or fractionated plasma products, such as clotting factor concentrates, albumin and intravenous immunoglobulin
Donations from family members and HLA-selected donors.....
Because of the sharing of HLA haplotypes, donations from
Family members pose a particular risk of TA-GvHD. Red cells, granulocytes, platelets and fresh plasma have all been implicated in TA-GvHD after transfusion from family members (Agbaht et. al.,2007), and there is an increased risk with donations from both first and second-degree relatives.
Several cases of TA-GvHD have been reported from Japan, where limited diversity of HLA haplotypes in the population increases the chance of a transfusion recipient receiving blood from a HLA haploidentical or HLA-identical donor. These observations are of relevance for patients receiving HLA-selected platelet concentrates from non-family members because of alloimmune refractoriness to random donor platelets. This would be expected to increase the risk of TA-GvHD, especially if the platelet donor is homozygous for one of the recipient HLA-haplotypes (analogous to donations within families or within racial groups of limited genetic diversity). A case of TA-GvHD in an immunocompetent recipient following transfusion of blood components from an unrelated HLA homozygous donor was recently reported , and four more cases were reported from Turkey in immunocompetent recipients who had received non-irradiated blood from relatives. The risk from HLA-selected platelets where the donor is not homozygous is uncertain. However, many transfusion centres now specifically maintain panels of homozygous donors for refractory patients, and in practice it is probably more reliable to recommend irradiation of all HLA-selected platelets, rather than risk the misallocation of some donations
Red cells....
Red cells can be irradiated up to 14 days after collection and stored for at least a further 14 days without significant loss of viability. Irradiation may result in reduced post-transfusion red cell recovery after more prolonged storage, although recovery is still above the minimum acceptable 75%. Irradiation of red cells results in accelerated leakage of potassium and an increase in the level of extracellular potassium. 'Top-up’ transfusions given at standard flow rates do not constitute a risk of hyperkaliemia, even when given to premature neonates. Potassium load may be clinically important in rapid large-volume transfusions, such as neonatal exchange transfusion or intrauterine trans- fusion. Routine removal of supernatant plasma and washing of irradiated red cells is not considered necessary but, if this procedure is undertaken, the washed cells should be transfused as soon as possible, ideally within 3 to 4 hours.
Free haemoglobin levels are increased in stored irradiated red cell components,but remain within acceptable limits. Irradiation has no clinically significant effect on red cell pH, glucose consumption, ATP or 2,3 DPG levels.
Platelets
Irradiation below 50 Gy has not been shown to produce significant clinical changes in platelet function.
Granulocytes
The evidence for irradiation damage to granulocyte function is conflicting, but in any case granulocyte products should be transfused as soon as possible after irradiation.
Recommendation.....
Irradiated components not used for the intended recipient can safely be returned to stock to be used for recipients who do not require irradiated components. The reduction in shelf life must be observed.
Clinical indications of irradiated blood components.......
(a) Definite Indications
- Directed donations ( from blood relatives)
- HLA-selected/matched platelet transfusions
- Granulocyte transfusions
- Intrauterine & all subsequent neonatal exchange transfusions
- Congenital cellular immunodeficiency disorders
- Allogeneic and autologus haematopoietic stem cell transplantation
- Hodgkin lymphoma
- Patients receiving nucleoside analogues for malignant or non-malignant disorders
- Patients receiving alemtuzumab for malignant or non-malignant disorders and transplantation
(b) Possible Indications
- Premature infants and infants weighing < 1300 gm
- All newborn infants
- Acute leukemia
- Non-Hodgkin lymphoma
- Patients with B cell malignancy who receive non-nucleoside analogue containing chemotherapy and/or radiotherapy leading to lymphopenia < 0.5x109/L
- T cell malignancies
- Patients receiving high doses of chemotherapy and/or irradiation sufficient to cause lymphopenia < 0.5x 109/L
- Patients receiving long term or high dose steroids as therapy for malignancies
- Aplastic anaemia receiving immunosuppressive therapy
- Massive transfusion for trauma
(c) No Indications
- HIV/AIDS
- Congenital humoral deficiency disorders
- Solid organ transplantation
- Small volume transfusion to neonates
![Advantages of X-Ray Irradiated Blood]()
Advantages of X-Ray Irradiated Blood
![Share on Twitter]()
![Share on Facebook]()